This article is primarily framed for family, friends and colleagues of multimorbid patients, to help build understanding of what your family member, friend or colleague may be trying to manage. It can be difficult for healthy people to understand the complications that can arise. The article may also be useful to new patients.
Some of us only have one condition or disease. A rather large number of us (see below) have multiple things to manage. I am one of those people! Usually it is not a problem, but the last few months have been interesting, to say the least.
Multimorbidity is common and becomes more common with increasing age
It is estimated that 38% of Australians (9.7 million people) had 2 or more of the selected long-term health conditions in 2022. This ranged from 11% of people aged 0–14 years to 79% of people aged 85 and over.
https://www.aihw.gov.au/reports/chronic-disease/multimorbidity-in-australia/contents/summary
Bear in mind I am writing from lived experience: the exact same things that I detail here are unlikely to happen to any other specific reader, but similar situations very likely will arise at some stage.
In my case I had been having a little bit of a problem with sleep and a nostril blocking at night for several years. I’d been to sleep specialists, done a sleep study, a CPAP machine was recommended. In August 2026 I was hospitalised with walking pneumonia (refer note at the end of the article). Gradually the nasal issues (and my sleep patterns) got worse.
In December 2026 I had my second ankle fused (I now have matching ankles). For some reason two things happened: 1) my blood pressure when crazy and 2) my nose blocking at night situation became intolerable over the following weeks. Yes, they popped me on BP meds while I was in the rehab hospital for the ankle.
Once out of hospital my GP (general practitioner) sent me off to see my cardiologist who did all the heart tests, showing my heart was fine. Titrated the BP meds. Even so, the BP kept fluctuating quite worryingly.
During this time the nose finally got the better of me. I walked into my GP’s office and said, “We HAVE to do something about this F**KING NOSE!” She referred me to an ENT specialist. At this point I still had not reached the 12 week post-op ankle check, and expected to have to wait to see the ENT specialist.
On March 24th I had my 12 week post-op and got the green tick for the ankle. Great! I’m free! That afternoon I got a call from the ENT office – they had a cancellation for March 26th, would I like it? Oh, yes please! I had ONE free day! March 26 I went to the ENT specialist who looked up my nasal passages into my sinuses and said, “I want you to go home, pack and head to the hospital. Now. I will call them and let them know you are coming.” His concern was I had a fungal infection in my sinuses and I discovered fungal infections in the sinuses are a little on the dangerous side. He was being responsibly cautious: fortunately for me I had a bacterial infection. In hospital for three days. Ultimate decision? I needed surgery. I thought my ankle was going to be the last surgery. Seemed not so.
To cut a long story short, the sinus surgery was scheduled for June 17th. During this period of time I had also seen my ophthalmologist and the decision was made I needed cataract surgery and fancy lenses. Those two surgeries (one eye each) were booked for July 27th and August 10th. All timed nicely, yes?
Then the rheumatologist threw a spanner in the works. I had my usual six monthly appointment with her on June 9th and naturally had the required blood tests a week beforehand. The blood tests showed a type of white blood cell, the neutrophils, were sitting at 1.2 and that is considered a little on the low side – especially when upcoming surgery is involved. So suddenly my June 17th surgery was delayed. A new tentative date of July 8th was set, but it would all depend on my neutrophils. I was to have blood tests every Saturday morning.
To top it off, my rheumatologist pulled me off both my arthritis medications cold turkey, in case one or both of them where causing the low neutrophil count. I was relatively fortunate as I didn’t suddenly have a jump in arthritis discomfort. Yes, my hands are a bit more problematic than usual and by late afternoon various muscles and tendons are not too happy, but I’m managing. I am back on one of the meds as of last Wednesday.
Thankfully my neutrophils did recover enough for me to undergo the sinus surgery July 8th. Great! However that then left me with the problem of the planned cataract surgeries. Because the ENT specialist would prefer I waited four weeks before any more surgery. July 8th to July 27th is not exactly four weeks. It is close to three weeks, but not quite!
So it was a stressful couple of weeks! However, I saw the ENT surgeon Thursday morning for the first post-op and he gave me the go-ahead to have the first cataract surgery done on Monday 27th July as planned. YAY! I was so excited!
Also saw my rheumatologist on Tuesday who also approved the cataract surgery timing. So I was very happy!
What I am not happy about is all this co-ordination between specialties was essentially done by me, the patient. Now, if the patient has a fully functioning brain, that’s fine, but mine was suffering from a lack of oxygen due to the sinuses. I somehow got my 8s confused at one stage and thought the sinus reschedule was for the 8th day of the 8th month. That did not help anyone’s planning! Finally I realised and got it sorted. I do think it would be a good idea if the specialists communicated directly in situations like this. I am NOT blaming my doctors, it is just how our system in Australia works. There needs to be improvement so the patient is not the primary communicator!
I have to say the brain has returned to normal because NOW I have a good oxygen supply! My O2 Sat and VO2 Max have both improved, my sleep has improved. My BP, while not yet back to normal, has at least stabilised. Even my Garmin watch tells me my oxygen levels are better!

My first (left) eye was done on Monday. It takes a few days for the eye to fully recover and the “new normal” vision to settle in, but as I write it is Thursday and I can definitely see light at the end of the tunnel (no pun intended).
At the moment (this is NOT permanent, just post-op), my day goes like this:
Morning:
- Disinfect hands
- Insert a drop of one med into the operated eye
- Wait one minute
- Insert a dop of the other med into the eye
- Flush the sinuses with saline solution
- Take morning medications, including Creon for the pancreas with breakfast
- Take and record BP for cardiologist
Midday:
- Lunchtime – take the BP med
- Disinfect hands
- Insert a drop of one med into the operated eye
- Wait one minute
- Insert a dop of the other med into the eye
- Take Creon with lunch
Evening:
- Take Thyroxine at least 30 minutes BEFORE dinner
- Disinfect hands
- Insert a drop of one med into the operated eye
- Wait one minute
- Insert a dop of the other med into the eye
- Take Creon with dinner
- Flush sinuses
- Spray a med up both nostrils
- Around 7:30 pm take BP readings for cardiologist
Before Bed:
- Disinfect hands
- Insert a drop of one med into the operated eye
- Wait one minute
- Insert a dop of the other med into the eye
- Affix eye guard over operated eye before sleep
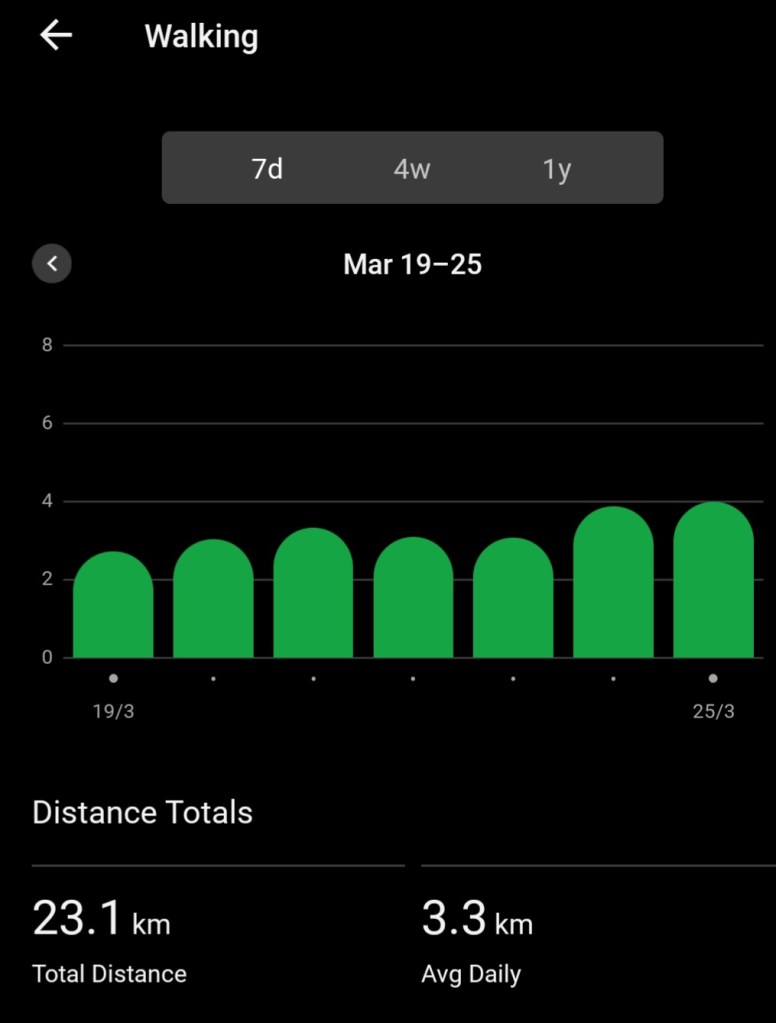
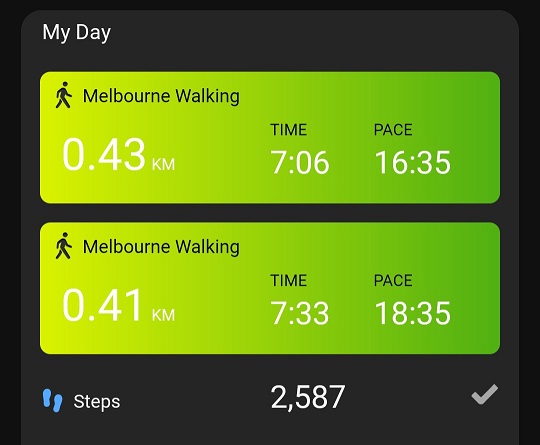
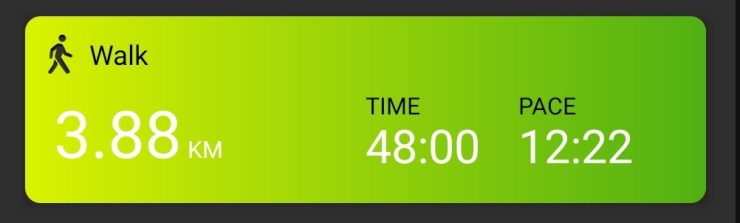
HOWEVER I am back to 7,500+ steps a day and 4 kms of formal walking. Not allowed heavy lifting yet, but might pop into the gym next week just to do a little light stuff.
I added up my surgeries. The right eye will be my 15th surgery.
Note re the walking pneumonia mentioned above. It is highly possible I did not have walking pneumonia but the issues I was experiencing at the time could have been related to my sinus issues. We can’t know for sure, but the diagnosis at the time was not conclusive. Hindsight can be a wonderful thing.
If you have a family member, friend or colleague who is a multimorbid patient, there are times when it is not fun and also not easy to co-ordinate. Please be understanding. There is also a gastroenterologist in the above mix, but that is a story for another day!