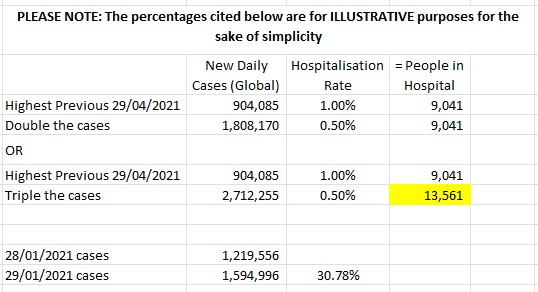
My random Tuesday thoughts: we are ignoring the Worst Case Scenarios. We are not planning ahead.
My previous writing on Covid-19: Covid Is Not Over
A related article re how society deals with the existing chronic illness population, which readers may find useful: Will Society Adapt? When? How?
“Cause for Concern”: Warning of incurable immune deficiency caused by #COVID from renowned 🇩🇪German Health Minister @Karl_Lauterbach. “Anyone who gets infected more often runs the risk of developing an incurable immune deficiency.”
— Eric Feigl-Ding (@DrEricDing) January 22, 2023
➡️Don’t risk infection!https://t.co/GwzOiDqqkK pic.twitter.com/frpzcNKyR2
I've debated for a long time about being public with this, bc it's heavy & I still haven't come to terms with it. But I have a rare pre-COVID datapoint so will do it, hoping it helps people:
— Hannah Davis (@ahandvanish) January 22, 2023
Right before I got COVID, I did neuro testing to see if I had ADHD.
1/ #LongCovid https://t.co/SBxDOx8Cku
I’m tired. I bring evidence and peer-reviewed publications about the economic damages from global heating, the heath and economy costs of COVID and the long term damages from Long COVID and nothing changes. Govt and the rich and powerful do nothing. Am I wrong? Should I give up?
— Tom Kompas (@Tom_Kompas) January 22, 2023
Come the cooler months, you’ll be wishing you’d kept everyone #DavosSafe! 🦠😷😡 #COVIDIsAirborne #CleanAir #vaccinesPLUS #LongCovid https://t.co/QorWud4N7H
— Desiree 💉😷🌬️ (@RainyDays8888) January 22, 2023
The days of being swamped with politicians talking about COVID already seem like a long time ago. But the virus continues to run rampant, making a lot of Australians sick and killing many, even if we don't seem to be talking about it publicly as much. #abc730 pic.twitter.com/f2hyVb9QXt
— abc730 (@abc730) January 23, 2023
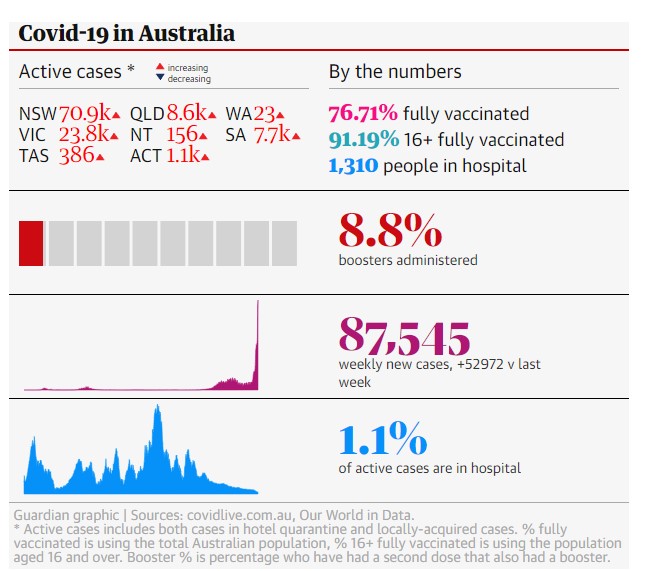
COVID pandemic now devastates Australia’s health with “unfettered” transmission. Life expectancy rapidly diminishing. Long COVID has cumulative public health/economic impacts. Experts tell @latingle we need urgent counter measures: masks, ventilation, vax, testing, data. pic.twitter.com/rc9z20homq
— Quentin Dempster (@QuentinDempster) January 23, 2023
COVID-19 Infection May Induce Fetal Brain Hemorrhages, Scientists Warn
— Jess (@MeetJess) January 23, 2023
« There's evidence of the virus in fetal brain tissue in instances of pregnant people passing the infection to their children » 💔
H/t @KatePri14608408 https://t.co/XPN17El9vS
You're getting kind of desperate now, guys. Arguing that air fit to breathe is rightfully a privilege of "billionaires, CEOs and heads of state" is not a good look. pic.twitter.com/IxoD0bFWFT
— Dr David Berger BSc MBBS MRCP(UK) FRACGP-RG DTM+H (@YouAreLobbyLud) January 23, 2023
"Long Covid now looks like a neurological disease, helping doctors to focus on treatments":https://t.co/DEf8x9uAio #LongCovid
— Hannah Davis (@ahandvanish) February 14, 2023
Interesting case report about the onset of CLL (blood cancer) following a covid diagnosis. The “but muh T cells” bros were at least right about one thing – we don’t know all there is to know about T cells & Covid-19. https://t.co/aXbsyx7fyR
— Arijit Chakravarty (@arijitchakrav) February 14, 2023
Please Share!
- Share on Facebook (Opens in new window) Facebook
- Share on Tumblr (Opens in new window) Tumblr
- Share on LinkedIn (Opens in new window) LinkedIn
- Email a link to a friend (Opens in new window) Email
- Print (Opens in new window) Print
- Share on Reddit (Opens in new window) Reddit
- Share on Pinterest (Opens in new window) Pinterest
- Share on Bluesky (Opens in new window) Bluesky
- More