

The Covid-19 Pandemic is horrible, frightening, life-threatening. Ignoring the very real practicalities does not solve the problems we face.
Health Systems Are Finite
Early in the pandemic we witnessed China build a hospital in ten days. I’m not aware of any Western nation that has even attempted similar. Even so, a hospital is bricks and mortar. No hospital runs without staff. While we can perhaps employ a secondment strategy to provide cleaning, food preparation and laundry staff, we cannot manufacture doctors, nurses, lab technicians, radiologists, pathologists and other health care staff overnight. Or, for that matter in ten days. It takes a good ten years to train a doctor and even then that doctor is not a specialist in pandemic related disciplines.
We, the people, yes us, we cry out for more doctors, more nurses. Where, exactly, are these health care workers supposed to miraculously appear from? It is not possible. There are limited trained health care workers in the world – not just here, in the world. Not enough to care for WAY too many sick people. We have to accept that as a fact.
Rapid Antigen Tests Need to be Manufactured/Distributed
We want more rapid antigen tests made available. Those have to be able to be manufactured in sufficient numbers. We don’t wave a magic wand and the tests just appear in pharmacies nationwide for purchase. The tests have to be manufactured under strict controls, packed, distributed. Staff are needed to run the production – do we have enough staff to run a 24/7 operation? Even if a 24/7 manufacturing process is running in existing production facilities, do we have enough of those? How long to build more?
Should the tests be free? I personally think so given the circumstances, but how is that managed?
There have been cases of price-gouging. Now it appears there is even more confusion, detailed well this afternoon by Luke Henriques-Gnomes in this thread on Twitter:
PCR Tests to be Collected and Processed
Again staffing issues apply when the sheer number of people needing testing are greater than ever anticipated. SHOULD the number have been anticipated? That’s a whole other question I’ll deal with later. At least the training requirements are not as onerous as for doctors and nurses. We could potentially increase testing capacity, but there will always be the physical constraint of staff availability. That is a fact we can’t change quickly.
More Infectious but Less Severe
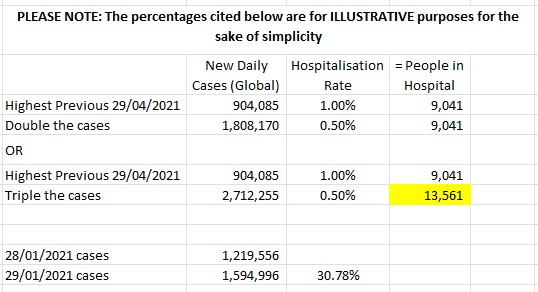
The numbers game. Each variant comes with unique characteristics. The general population can be confused if the messaging isn’t clear. As the scientists reiterate, a small percentage of a larger number may be larger than a large percentage of a smaller number. The below quote is Dr. Abdul El-Sayed, epidemiologist and former Detroit Health Department executive director speaking to CNN.
“Just because the per-individual risk of severe illness may be lower, that doesn’t mean on a societal level Omicron doesn’t pose a real risk,” he said. “Even a small proportion of a relatively large number can be a relatively large number.”
https://edition.cnn.com/2021/12/28/health/is-it-cold-flu-or-covid-wellness/index.html
This is a simple example I whipped up to illustrate what this can mean. The percentages used therein are for ILLUSTRATIVE purposes only. As we can see, triple the cases with half the requirement for hospitalisation still results in MORE patients needing hospital care. The new case numbers jumped 30.78% from December 28 to December 29. Yes, there are reporting delays and all sorts of other variables to the reported numbers of cases on any given day, but they are indicative of what is happening. The most important variable is these are only the tested people: how many globally are not being tested? How many do we not know about at all?
I do note that as of December 30, 1.1% of active cases in Australia are hospitalised. I have been unable to confirm whether this includes Hospital In The Home numbers. Note the source below updates daily.
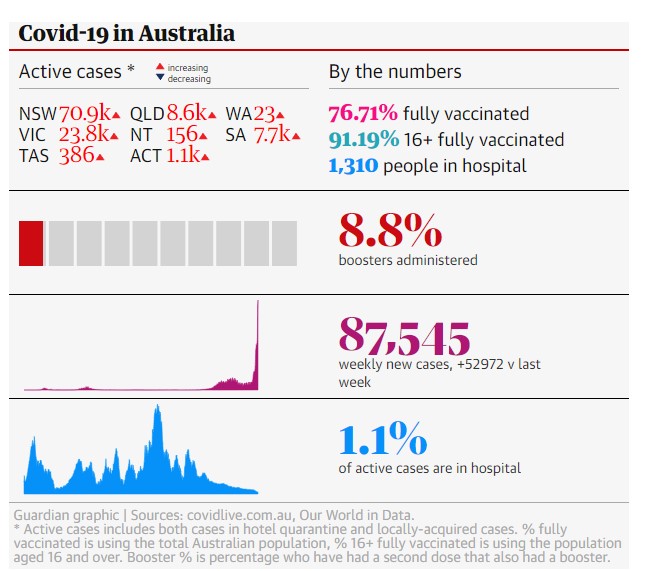
Edited January 8 to add: now some days later, compare the same data. We can see we now have three times the number of people in hospital, but that is a lower percentage of currently active cases.

The Science, NOT The Politics
Yes, the damn politics. The politics has got to stop and stop now. Right now. This is a global disaster and there is no place for politics. If you aren’t part of a SAFE solution, you’re part of the problem. Point scoring off the other side isn’t helpful: and that applies across the board. Personally, I’m not interested in what political colour you are, you are elected to represent us.
As for threats of war and similar “business as usual” inter-nation “disagreements”: THIS IS NOT THE TIME.
LISTEN TO THE SCIENCE. That’s all I ask you to do. Listen to the science.
There is also a simmering question of a particular religious ideology impacting political decision making. I am avoiding that topic today, other than noting yes, that question quite legitimately exists.
Like it or Not, it IS a Numbers Game
During the last pandemic, the 1918 Pandemic, the global population was less than 2 billion. Now it is 8 billion.

During the 1918 Pandemic one third of the world’s population was infected. It is estimated the population in 1918 was 1.8 billion. Everything is relative: in 1918 our population was much lower, but we also likely had less health care workers per head of population than we do now in 2021. It was also a different type of illness. Covid-19 puts people in hospital for long periods. People technically recovered from Covid-19 remain very unwell for long periods or are permanently disabled with Long Covid.
Back to the numbers. One third of our current population is 2.66 billion people. We already know people can catch Covid-19 more than once, that alone increases the numbers. Yes, we have vaccines and those vaccines have been shown to reduce the severity of the disease. On the other hand, Covid-19 has variants. Those variants may evade vaccines and be harder for current tests to detect.
Are we safe to assume that Covid-19 will not infect a greater proportion of the global population that the 1918 Pandemic did? I don’t think so. SO FAR we have been fortunate. In the two years of 2020 and 2021 our reported total cases are only 284,906,146 which for those into numbers is just over a quarter of 1 billion or 28.49% of 1 billion. That is a long way from 2.66 billion.
Oh, but we have better science now than in 1918? True, we do. Very much so. We managed to get vaccines up and running in basically 12 months, give or take. An astounding achievement. We have dramatically improved treatments of Covid-19 patients and continue to learn. However, there are far more of us, living far more densely and travelling far more widely than in 1918. Those factors work in Covid-19’s favour. Not to mention the anti-vaxxers who risk not only themselves, but society in general.
Then we loop back to the Health Systems are Finite aspect. The health care workers we do have cannot work 24/7, it is not possible, none of us can. If the number of cases requiring hospitalisation or Hospital In The Home or whatever care type might be developed in the future, exceed our health care system resources, we have a problem.
I’m not being alarmist but I see way too much lack of understanding of the numbers.
- “Just get more health care workers!” – WHERE FROM?
- “Triage the patients to another hospital.” – And when/if all the hospitals are in the same boat?
- “Provide free tests now!” – Where is the supply coming from? It takes time…..
- “Fix the overloaded PCR testing, stop the queues!” – How? Where are the staff coming from? Are there enough test kits?
What IS needed is an acknowledgement by politicians and understanding by the general public, globally, that in a worst case scenario we could be trying to treat an INORDINATE number of people. Australia’s population is 26 million in round numbers. One third of 26 million is 8.66 million people. Of that 8.66 million people, up to 37% could be left with some form of Long Covid. That equates to 3.2 million people.
I certainly hope we don’t reach the levels of the last pandemic – but I suggest it is a very dangerous assumption to assume we won’t.
Close Contact Definitions
I refer readers to the OzSage report linked below, where this point is discussed.
Today the Queensland Chief Health Officer stated the definition of close contacts had to change or the state would cease to function, everyone would be in quarantine.
Not much will function too well if too many people are sick, either. New South Wales discarding spread mitigations and protections when they did was grossly irresponsible.
Long Covid
Then there is Long Covid to consider. So much is as yet unknown, but the more I read, the more concerned I become. I’ve written other articles about chronic illness and society, so I’m not going to repeat myself here. Suffice to say the same problems will exist, but for more people. What are the politicians doing about modelling the social, health and economic costs?
A Guardian article today addresses the issue well: Long Covid is the elephant in the room, but it seems invisible to Australian politicians. The existing chronic illness cohort seem invisible to many politicians, so I’m not surprised they’d have to be dragged kicking and screaming to acknowledge what could be a major increase in numbers.
This UK Long Covid patient has detailed his struggles on Twitter. One of many.
The OzSage Report: 10 Key Points
I implore everyone to read the OzSage Report. Here is Point 5 to encourage you to click on the link below.
The rhetoric that case numbers ‘do not matter’ is incorrect – particularly in the face of the Omicron variant. Daily case numbers are now 10 times higher than during the Delta wave and may be 100 times higher in January. Even if hospitalisation rates are lower with Omicron compared to Delta, a halving of hospitalisation rates with a 10-fold or 100-fold increase in cases will still translate to a high burden on the health system. This is likely to overwhelm the health system, with regional services at particular risk.
The trajectory of observed data suggest that hospitalisation and ICU occupancy are on a steeply rising trend and anticipated to exceed earlier peaks quite soon. In other words, optimistic assumptions about the impact of the Omicron variant on hospital admissions are unrealistic.
https://www.theguardian.com/australia-news/2021/dec/30/the-ozsage-report-10-key-points-from-its-critique-of-australias-covid-response
Should We Have Seen This Coming?
The answer is yes, we should have. Humans got too wrapped up in The Economy and Growth (I wrote the below article in August, 2020) and forgot we are really just another species of animal on the planet.
Humans are Earth’s chronic condition. We destroy at will. We see our species as the pre-eminent beings on the planet. Although many believe in a God or Gods in the heavens, here on Earth the human species is all-powerful.
The Gods Brought to Their Knees by the Invisible
Scientists have been warning us for years, but we didn’t listen. We didn’t prepare. In fact, in some ways, we deliberately de-prepared: sold off the Fairfield Infectious Diseases Hospital, for example.
In many ways it would be impossible to plan for the sheer numbers. We can’t have excess trained health care workers sitting around idle for generations, or hospital buildings lying idle. Equipment becomes outdated, supplies pass their use-by dates. Vaccines and tests have to be developed specific to the pandemic. The logistics of it all are difficult to grasp.
But we should have seen it coming. For the politicians to act so surprised is ridiculous. We should, as a species, globally, have been prepared to some degree. Not perfectly prepared, for that would be impossible. Yes, in a pandemic there will be unavoidable loss of life, there will be economic losses, there will be disruptions to travel, education, trade, life as we knew it… Yet we could have been better prepared, not only by having plans at a macro level, also psychologically at an individual level, for the disaster that is still unfolding.
There are no miracles.

Not at all a rant, but a very well argued and well expressed article. I hope you are not just preaching to people in he choir, like me!
LikeLiked by 2 people
Thank you Melvyn.
LikeLiked by 1 person
This is very informative Robyn, and says it all.
LikeLiked by 2 people
Thanks, Robyn, glad you found it useful.
LikeLiked by 1 person
[…] https://limberation.com/2021/12/30/pandemic-practicalities/ […]
LikeLiked by 1 person