As I sat down to write this article, I realised the last article I published was August 27 LAST YEAR! I have been quiet for a very long time. Sometimes, in the chronic illness world, this happens. Our priority at all times MUST be project managing our situation. If nothing else, this article will demonstrate how the unexpected can happen and somehow we still have to manage it all.
What started with the August 2025 trip to hospital turned into a stretch of challenging time. When I got home from hospital I was still recovering to some degree. So that was my priority. I really had no brain waves about topics to write about either, as my focus was on getting my Movement Is Medicine back on track. On October 26 I received a call from my brother: the doctors had given him two weeks to live. I spent the rest of the day organising flights and left for Aotearoa New Zealand the next day. My sister had passed away in 2023, losing my brother as well so soon is so sad. I was notified of his passing as I was being discharged from the rehab hospital (see below). While I am very sad to have lost my brother, I am relieved he did not spend months in severe pain.
I returned from Aotearoa New Zealand in November and starting physically preparing for the scheduled second ankle fusion (that took place December 2). Readers who have had an ankle fusion or read about my first ankle fusion will know that while the final outcome is fantastic, the post-op period is a nightmare!

In summary:
- 2 weeks in a plaster cast, operated foot elevated 23 hours of every day (in a rehab hospital)
- 4 weeks in a fibreglass cast, non-weight bearing so on a knee scooter
- At the 6 week mark, x-ray, review by surgeon, if all good promotion to a moonboot
- 4 weeks in a moonboot, with crutches for the first 3 weeks as the weight bearing is increased slightly each week
- At the start of week 11 you can actually migrate to runners! Yay!
- At the end of week 12 another review by the surgeon and hopefully you are set free: with some restrictions.
Of course, showering is a challenge. Non-weight bearing, so a shower chair is needed, and of course the cast has to be wrapped in a couple of rubbish bags. Tip: so you can find the start of the tape after the shower, I do a little fold over bit as shown below.

So it is a long 12 weeks. Also, this time it was my right foot, so I had an extra four weeks that I couldn’t drive than with the left foot. For Americans reading this, we drive on the other side of the road. Can’t drive in a moon boot!

I wasn’t sure why, but even then I just didn’t feel up to writing. I was to find out, at least partially why, rather quickly.
On the same day I saw the surgeon for my green tick, I had a GP appointment. My main topic for her was, and I quote, “We have to do something about this f**king nose!” I’ve had problems with the right nostril blocking at night for about two years – it is why I bought an adjustable bed base. The blocking seemed to have worsened since the surgery. I was well and truly over it. My GP referred me to an ENT specialist. Through sheer luck I snagged a cancellation slot on the Thursday instead of waiting the usual three months to get in to see a specialist.
By Thursday afternoon I was back in hospital.
A different hospital, but still a hospital. The ENT specialist had popped a camera up my nostrils and wasn’t happy with what he saw. He was concerned I may have had a fungal infection. The less dangerous possibility was a bacterial infection. On reflection, I think because he had never met me before, he stressed the risk of a fungal infection to ensure I’d go to hospital. So I went home, packed (forgot slippers of all things) and a neighbour kindly drove me to hospital. The specialist had called the hospital and spoken to the ENT department, but I still had to go through ED (Emergency Department). They couldn’t find me a pillow. A minor but annoying complication. Blood tests, nasal swabs, IV antibiotics and steroids followed. To cut the story short, turns out it was bacterial, not fungal. I will be reviewed on April 17, but at this stage the plan is…..more surgery. On my sinuses. Wonderful.
I come home from the hospital with two nasal sprays, antibiotics, steroids and a nasal/sinus wash. Great. And I really wasn’t feeling too well. Again writing articles dropped down the priority list.
An added complication has been my blood pressure (BP). Now, I’ve always been rather proud of my perfect blood pressure. There is one non-steroid anti-inflammatory medication that will raise it, but I don’t take that medication any more. However, there I was in the rehab hospital (December) and my BP was sky high. Even as I write, it is still not back to normal, but there has been considerable improvement. Yes, I am taking BP medication *throws arms in the air*. This has never happened with any of my other surgeries (both knees, other ankle, bi-lateral foot surgery plus a number of “removals” of “optional” organs).
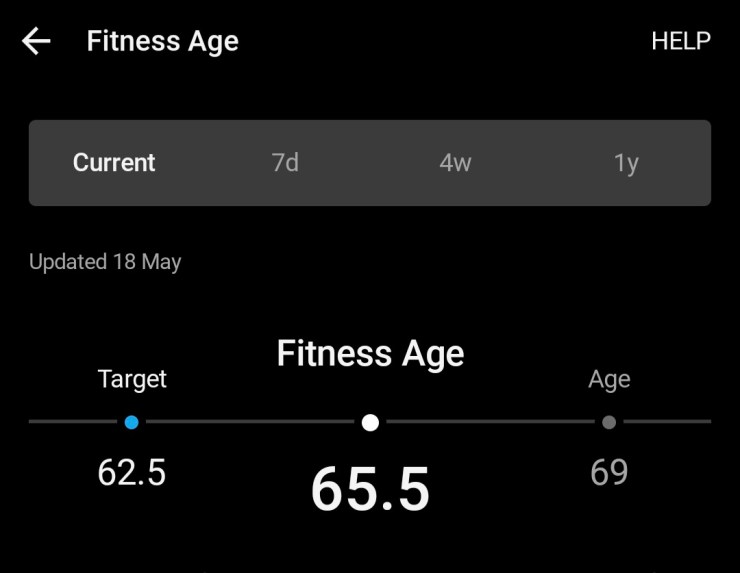
Even my trusty Garmin smartwatch has been telling me my activity assessment is “Strained”. In all the years I’ve been wearing Garmin, I’ve never before been told I was straining to achieve my walks or anything else! Now I was. This week, I’m finally back to “Productive”. Yay!

It seems the stress of surgery on my immunosuppressed body may have allowed the bacterial infection to get a better grip on my nose/sinuses. My VO2 Max had dropped three points which I initially put down to lack of activity, but I think the nasal issues have not helped. The BP we initially thought may have been a reaction to the anaesthetic but any reaction should be well and truly resolved by now (almost four months later). So yes, I’m getting checked out by my cardiologist in April. Last time I saw him, some years ago, the problem was low BP.
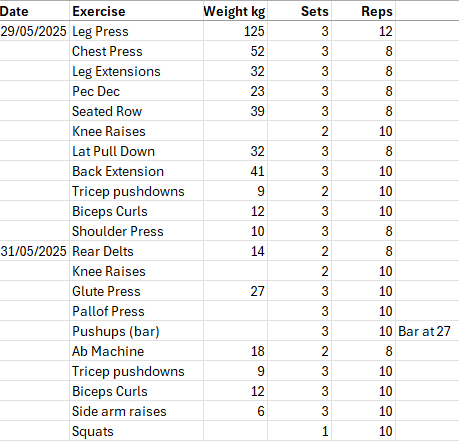
Back to the ankle fusion! I knew what I was letting myself in for this time. I organised my own knee scooter that was the right height for me. I had suitable clothes to fit over the casts from the previous surgery. I still hated the knee scooter, the immobility, the frustration. However, knowing I had an extra four weeks of no driving this time, I bought dumbbells so I could keep doing upper body exercises at home, plus I had rehab exercises for the legs from the physio. I had even taken my dumbbells into hospital with me, as the heaviest dumbbell they have is 5 kilograms.
It took a bit longer for this ankle to reach the totally pain free stage, but i think that was because the sinus infection slowed down the healing. It is fine now, I’ve even got back on the leg press machine (at a very low weight!).
Even after all that, this week I discover I need cataracts removed and I’ve chipped the front off a tooth crown so off to the dentist next week. I need a holiday from health stuff! Although I have to say I did like the morning tea cake with the little blue flower (at the top of this post)!
What kept me sane all this time? To a large extent, the lovely people I puzzle with on BlueSky who, although they didn’t know it, were helping take my mind off all of the above. They made me smile. Thank you all.