Humans are Earth’s chronic condition. We destroy at will. We see our species as the pre-eminent beings on the planet. Although many believe in a God or Gods in the heavens, here on Earth the human species is all-powerful.
This year the God-like species has been brought to its knees by something it cannot see. A tiny, minuscule, virus. So insignificant, it is not considered to be living. Yet this unalive molecule coated in protein has shut businesses, grounded air traffic, overloaded the health systems of several cities and killed nearly 700,000 people (at the time of writing). We wear masks, socially distance and in Melbourne we are now under a curfew. Many work from home, many are not working at all. The human worship of the great God Economy has been called into question most dramatically by the state of our aged care homes.
Despite great advances in science and technology, humans are losing the battle. The front-line defence, healthcare workers, are dying.
Some leaders are performing brilliantly trying to save and protect their constituents. Local leaders Dan Andrews of Victoria and Mark McGowan of Western Australia spring to mind. The New Zealand Prime Minister has achieved what many deemed impossible. Others are intent on using the virus as an excuse to denigrate these leaders and undermine their efforts. Tim Smith and Tim Wilson are two examples in Australia.
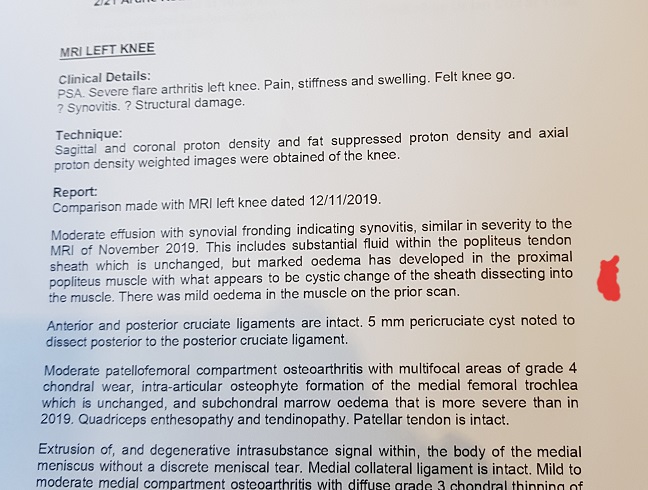
I am the beneficiary of advances in medical science. I have a prosthetic knee and I’m on a clinical trial. If I was living 200 years ago it is possible I’d be severely immobile, yet in 2020 I am lucky enough not to be. While I recognise the wonderful things we, as a species, are capable of, I also recognise how damn stupid we can be.
I don’t need to provide links, nor do I want to, highlighting the ridiculous conspiracy theories and “my rights” people. The inability of some to accept the existence of something they can’t see is one problem. The selfishness of the “it is my right to go maskless” brigade is another. The lack of numerical literacy, where people cannot comprehend growth rates and infection rates, is a problem.
At the moment there is much talk of vaccines. I hope as much as anyone that a vaccine is developed: I am also aware it will be the first coronavirus vaccine. To date we have not developed one, partly because coronaviruses have not previously been so contagious and deadly/damaging. Then there is the question of availability. Will only the rich be able to afford any vaccine, or will a vaccine be made available to all? The great economy, you see, would not like a free vaccine.
The human species has been brought to its knees. Not by aliens, not by flood or fire (yet, that’s coming) but by an unseen molecule. Humans are reminded despite our belief in our own pre-eminence, that we are vulnerable. Humans can, indeed, be on the receiving end of the same brutality humans dish out to other creatures on this planet. We steal and destroy their habitats, we shoot them for sport, we really don’t care if other species become extinct through our actions. Now we know how it feels. We’ve lost the freedoms we took for granted: the freedom to crowd supermarkets, to fly to the other side of the world on a whim, to get a haircut when we feel like it.

We ignored the beauty and fragility of our world because we did not feel fragile. We redefined beauty to be tall skyscrapers, fast cars and electric lights.
Human’s biggest enemy has always been other humans. Wars. Killing each other. Now humans have a new enemy. It isn’t the first and according to science, this will not be the last.
I wonder if this is the wake-up call we need. Time to re-evaluate our way of life. Re-evaluate our disrespect for the flora and fauna with which we share this planet. Re-evaluate our worship of the God Economy.
Managing the economic and social costs of the survivors suffering chronic illness is going to be a challenge. As I have written before, as a society we do not cope well with chronic conditions, I worry that many are going to suffer greatly in the years ahead.
How we cope with the aftermath of this pandemic is going to be a major test of the humanity of the human species.