While the Cancer Council reminds us ALL to ensure we have adequate protection from the sun, those of us with chronic conditions need to be extra, super duper, especially careful.
One of my drugs comes with this little warning sticker.
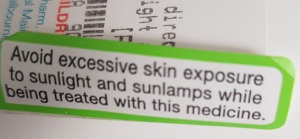
Let me tell you, that word “excessive” can be very open to interpretation. For some of us, that can be a whole 10 minutes. While I don’t enjoy sharing bits of my body openly like this, in the interests of education, I am doing so here. This is a snapshot of one of my breasts, I hope suitably cropped to retain a health focus!

That was THREE weeks after the actual exposure. I finally went to the pharmacy and asked if they had a cream I could use.
Knowing what else I was on, the pharmacist, in a very firm voice said, “Will you just go to the doctor? Please?” I mumbled, grumbled and complained, but I went.
Doctor says, “I need to send you to a skin specialist.”
I reply, “NOOOOOOOOO! I see enough specialists already! Can’t you prescribe something?”
Anyway, the point is: SLIP, SLOP, SLAP. Extra!
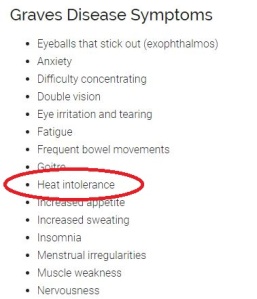
Sometimes it is our meds, sometimes it is the conditions. Sometimes it is a combination. Check your meds, check the symptoms of your conditions.
Hyperthyroid has heat intolerance as a symptom.
Here is just one paper on PubMed discussing sunlight interacting with drug medications.
The interaction of sunlight with drug medication leads to photosensitivity responses in susceptible patients, and has the potential to increase the incidence of skin cancer. Adverse photosensitivity responses to drugs occur predominantly as a phototoxic reaction which is more immediate than photoallergy, and can be reversed by withdrawal or substitution of the drug. The bias and inaccuracy of the reporting procedure for these adverse reactions is a consequence of the difficulty in distinguishing between sunburn and a mild drug photosensitivity reaction, together with the patient being able to control the incidence by taking protective action. The drug classes that currently are eliciting a high level of adverse photosensitivity are the diuretic, antibacterial and nonsteroidal anti-inflammatory drugs (NSAIDs).
Not all people will be susceptible. Two people could take the exact same medication and one be photosensitive and the other not. The same with symptoms of conditions: not everyone has the same symptoms. Unless you know for sure, it pays to do your research BEFORE you get over exposed.
My arm has had a problem for some time, as it keeps getting exposed. I initially thought I had got sunburn on that arm driving around on a beautiful winter day in August with the roof down on my car. It just never would heal completely. I have noticed a vast improvement since I stopped one of my drugs recently. I am monitoring progress while still applying the treatment the dermatologist prescribed after I was diagnosed, via biopsy, with photosensitive eczema.

That photo is not particularly bad, but I think you can see the lesions. While sun exposure would cause it to flare up, it is/was also heat sensitive: when I work out at the gym, those areas would become bright red.
In Cancer Council ACT’s recent media release, Dr Andrew Miller, President, Australasian College of Dermatologists is quoted:
“Melanoma rates in Australians aged 40 and under are dropping and the children of today are our most SunSmart generation ever. However, it’s a real concern that sun protection behaviours overall don’t seem to be improving and that over 2.7 million Australians are putting themselves at risk of skin cancer by getting sunburnt on summer weekends.”
A media release from Cancer Council Victoria states:
New data from a Cancer Council Victoria survey shows more than a third of Victorians do not know the correct indicator of sunburn risk – putting themselves and their families at risk of sun damage and ultimately skin cancer.
The survey found 22% of Victorian adults aged 18-39 incorrectly selected temperature as the most useful measure to calculate sunburn risk for the day, while 8% thought cloud cover, wind conditions or humidity were sunburn indicators, and 9% didn’t know which measure to use.
Just 61% were able to correctly identify the sun protection times or UV level as the best measure to determine sunburn risk.
Of course, all of that is for normal people! We spoonies have to be extra careful.
I use a Cancer Council sun protection that is non-greasy.

I initially bought the spray, but I find the nozzle clogs up quite quickly, so I have moved to the cream in the tube. Yes, my cat was trying to get into the photo – she gets into EVERYTHING. The non-greasy is better for work, although that may be all in my mind.
I also have a special dermatologist recommended cream for my face.

If I don’t use it, I can go from perfect skin to THIS horror over night. Go to bed perfectly fine, wake up horrified. I’ve learnt my lesson.

Have I scared you yet? I hope so, that was the entire point!
Go check your meds and your condition symptoms and SLIP, SLOP, SLAP not just in summer, all the time. I got my arm damage in August.
Do I let any of that stop me being active? No. While my skin may react to sun exposure and heat, I can manage that with suitable sun protection. If I don’t keep moving, I can’t manage my pain. The moving, exercising wins! I will say my gym is in a basement, so I’m safe down there.
Here is proof of me swimming, for no other reason than one of my readers complained on Twitter I had used shots of the pool I go to, but he never saw proof of me actually IN the pool. @MlsMichael, here is your proof. From today. Before the thunderstorms.
Most Australians already know what “Slip, Slop, Slap” means, but for overseas readers:
- Slip on a t-shirt
- Slop on sun screen
- Slap on a hat