I’ve had a weird day. Even for someone who has had this disease for ten years, this is a weird day. I’m writing about it for three different audiences:
- Medical professionals, because this is the stuff we never get to cover in an appointment with you
- Friends, family and colleagues of chronic illness patients, to provide some insight into what your friend, family member or colleague may be going through
- Other chronic illness patients – sometimes we can feel as if we are the only one having particular experiences.
The overall situation I describe here is not unique to psoriatic arthritis, but some aspects will be. As that is the disease I have, that’s what I am writing about.
Let’s get into it. This morning I woke up at 6:15 am feeling like a broken doll. I had sore fingers, sore wrists, sore upper arms and a sore neck. Thankfully, my lower body seemed perfectly fine. There was also a very blah feeling. Malaise? Not sure I was quite at the malaise stage, but I certainly didn’t feel like singing and dancing.
By about 10 am I thought to myself, “Oh, I think it is starting to lift!” Tossed up whether to shower or have a coffee, decided om the coffee first. By 12:36 pm I was actually showered, dressed and had lipstick on (I mean, really, did you doubt the lippy?). Yes, the above photo is me, today, AFTER I felt human.
I remember thinking to myself as I drove to the gym at 1 pm, “This is like two completely different days in one.”
At that point I felt like I could climb Mt Everest. OK, not quite, but the difference was SO stark. Unusually so. This slow, crappy start to days is not unusual, but often the bad is not so bad and/or the good is not such a massive improvement as what happened today. I really felt like a completely different person, physically.
I think there is a tendency for the general population to understand that mental health conditions may fluctuate, but tend to perhaps think of physical conditions as being more consistent in presentation – not totally consistent, of course, but shall we say mostly more consistent. Some are, I agree. Some are not.
I had steroid injections in my shoulders on Thursday so had deferred going to the gym out of an abundance of caution. I really wanted to go today, but waited to see what my body decided to do. My favourite gym leggings helped, of course.

Ultimately, I had a good workout.
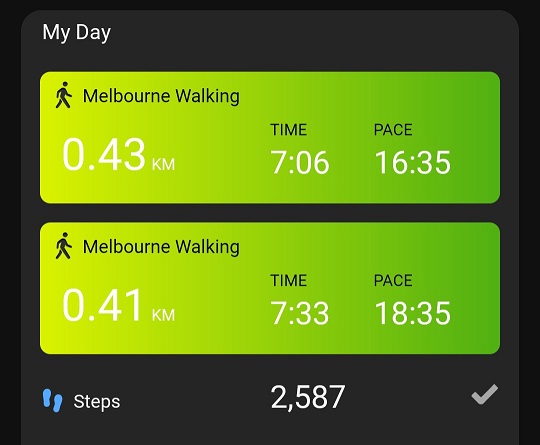
- 1 km on the treadmill as warm-up
- Leg press
- Chest press (left shoulder clickity clicking on this)
- Leg extensions
- Seated row
- Vertical knee lifts
- Triceps
- Leg curls
- Back extensions
- Lat pull-downs
The free weights area was a little overpopulated so I skipped biceps and shoulder press – they can wait for next visit.
As I write, it is 4 pm. I’m pretty much a “healthy” person.
This was a GOOD day, in that I came good as the day wore on. Sometimes we are not so lucky. OR we may wake up already feeling ready to take on Mt Everest. The issue is, we never know until we open our eyes in the morning. One morning recently I woke up unable to bend my left knee. Another day (some time ago) I was driving when I suddenly realised I couldn’t turn my head to the right (to check for traffic). On both occasions the rest of me felt fine!
This unpredictability makes planning life difficult. In time, my new medication hopefully will make everything more stable: it is still early days. But for many of us, today (or variations thereof) is what we live with. It can be hard for those around us to understand, especially when we do not LOOK sick. The invisible illness scenario.
The recent shoulder issue is a classic example of that. I LOOK fine. But reaching forward to put stuff in the microwave, or turn on a power switch, or turn on a tap were problematic. Lifting my arms about chest height, or anything involving internal rotation. Getting dressed was super challenging. Let’s not even discuss bras! But I LOOKED fine.
I can generally go with the flow because I’m retired. I’m not trying to get kids ready for school or meet a work deadline. I’m not trying to cook for a family of six. I really feel for those patients who have these types of responsibilities.
To my fellow patients – you are not alone. There are many of us out in the world facing similar challenges.
To everyone else – just because you can’t see something, doesn’t mean it isn’t there. You aren’t living the daily, sometimes even hourly, challenges. Support your family member, colleague, friend or patient.
Me? Hey, I just hope tomorrow is as good!