Maintaining our upward trajectory in managing our conditions can run into obstacles every now and then, one of those rocks in the road can be a change of treatment. We need to ensure we don’t let our progress to date slide away while at the same time ensuring we give ourselves physical and emotional space to deal with the bumps in the road.
What I have learnt from my own recent experience of changing treatment, is this.
Triple Check Any Timing Advice
You may get different advice from different practitioners involved in the treatment, if there is more than one practitioner (as is so often the case). If you have to make plans, such as time off work or someone else to care for your children, triple check! My example is I was originally told I would need to be isolated for ten days. I made plans around that advice, such as leave from work. A week before the treatment, I discovered it was five days for work, fourteen days for family/friends over five years of age who were not pregnant, and twenty-eight days for under-fives and pregnant women (which of course can affect working arrangements depending on your job). My isolation specifications are all around time and proximity: preferably not closer than two metres for more than 15 minutes a day.
The point is, when we plan for child care or time off work well in advance, we need to be confident we are planning correctly. I haven’t got to the root cause of why the patient gets different advice from different parties, just warning it is possible, so watch out for it!
Ask About Your Specific Activities
While there were pages of frequently asked questions provided, not one of them addressed swimming or going to the gym! In my case I was allowed to swim on Day 3 and go to the gym on Day 5, provided I took my own towel and kept two metres away from children. I needed to specifically ask about exercise related activities though – something I think is an improvement that could be made in the documentation!
The medical profession are certainly quick to tell us exercise is important medicine (obviously I agree) but then leave all mention of exercise activities out of the FAQs.
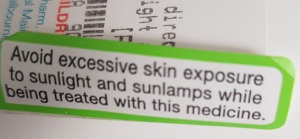
Make Sure You Are Advised Of Any Possible Health Effects
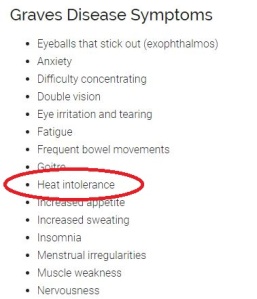
Perhaps due to my own naivety I expected my change of treatment to be relatively smooth. In reality, it really has been smooth, I certainly can’t complain too much! Let’s say the effects can be disruptive to your normal routines. I had a period of feeling, as an English friend says, “rough”. Rather a good description, really, rough! While every situation is different because there are a myriad treatments out there for a myriad of conditions, I found I had an increase in nausea/lightheadedness attacks (which are quite debilitating) and I started to feel RA pain in my hands – this I believe due to the fact my thyroid was having a field day running wild while waiting for the radioactive iodine to work its magic. A thyroid on a binge can exacerbate RA symptoms. Lethargy/fatigue reared its ugly head as well for a few days.
This is being resolved by my going back on my old thyroid medication at a half dose – not an unusual recommendation in my situation, but every case is different. This is an EXAMPLE only!
A stroke survivor friend of mine recently ended up in hospital as his body adjusts to a change in medication. Very different medical cases, he and I, but similar results in that a change of treatment lead to a changed health experience, albeit temporary.
Make sure you are aware of what you might expect and the steps to take to mitigate any unpleasant effects. I knew I could call my endocrinologist for directions, I knew what to watch out for and my GP is watching over me.
Keep Moving As Much As You Can
I will be the first to admit when the nausea/lightheadedness kicks in, there is not much moving of any sort to be done. I am still constantly surprised at how debilitating it is: there is NOTHING I can do when it hits. Apart from take anti-nausea medication. Other patients I have spoken to say similar. No pain, just the awful, all-consuming feeling of utter “OMG, I have to lay down”.
In my case, the overactive thyroid, probably in conjunction with the low iron (lots of chicken and egg stuff here, I have to say) definitely affected my muscle strength/tone. I was very keen to get back in the gym as soon as possible as I know my conditions result in the loss of previous strength gains very quickly. I’ve worked very hard to be able to do what I do now, I don’t want a ” one step forward, five steps back” situation! I actually haven’t made it to the gym since the treatment change. I was heading to the gym yesterday, but I got waylaid buying a dress – not the advice I would give my clients, but I’m excusing myself on the basis I did walk 8,295 steps in the process of said retail therapy! So back into it today!
I have been swimming, although that was before I started back on the medications and I could only manage 500 or 600 metres before I felt completely wiped out. The point is – do as much as you can, while at the same time being cognisant of the fact your body is going through an internal adjustment. Making the judgement of how much is not enough or too much is a skill that needs to be developed – if this is a first time experience for you, you may need some professional help in making the right choices. Listening to your body and common sense are pretty good decision making aids. Just don’t fall into the trap of using any side-effects of the treatment change as an escape clause, because you will likely regret it later.
I did definitely find I was getting stiffer over the worst few days – reminded me very clearly of WHY I started all this exercise stuff in the first place! I don’t like that stiffness one little bit. Very glad to be getting back to my definition of normal now!
Summary
A change of treatment is often recommended for a variety of reasons. I had a change of RA medication in 2016 with no rocks on the road. This time has been a bit different. I am sure over the coming years I may have other treatment adjustments or changes.
Each change may or may not bring temporary changes to our experience. Our goal during these times is to minimise any reversal of our quality of life gains to date.
As mentioned above I felt stiffness starting to return over a few days of relative inactivity. I was stiff getting out of bed, stiff getting off chairs and was finding getting out of my car a bit of a challenge. THAT, if nothing else, is enough of a trigger for me to GET MOVING! The last thing I want is to be unable to get in and out of my car!
Be prepared, plan well, use the medical support available and most of all KEEP MOVING!
Good luck!