No, I don’t have one, at least not yet. What IS she on about, I see you wondering. Let me recap. Back in May 2023 I wrote about Crossing My Fingers – Again. As it turns out, I was counting my chickens before they hatched. I saw my rheumatologist a week before my (latest, second) knee surgery and the decision was made no, the medication I was on was not working. HOWEVER, because my knee surgery was looming, I couldn’t start the next, the eighth medication, until ten days after my surgery due to infection risks, it being an immunosuppressant. This new medication can take twelve weeks, roughly three months to work – or more. Here we go again, I thought.
I started the new med in the second week of August. About three weeks ago I mentioned to my GP that if anyone were to ask, I would say the new medication was working about 50%. I qualified that statement by saying, “But the question is really, 50% of what? 50% of the maximum efficacy of the medication, or 50% of what I expect?” Hey, I’m an accountant – percentages make sense to me!
At my rheumatologist appointment this week, I relayed that conversation to him. I then added, for example, what percentage of normal can I expect to feel? 100% normal? 80%? Do we have a ballpark number? He sat back in his chair and said that was a very interesting question, he’d never heard it expressed like that. He told me, “We always aim for 100%, but don’t always make it”.
It is interesting to note that in cited clinical trials, on my new medication at the one year mark 68% of patients in the trial experienced “less joint pain and swelling”. Only 68% of patients? Only “less”, not “it had all gone away”? I’m not linking to the study results as I don’t name the medications I take simply because what doesn’t work for me might work perfectly well for other people and I don’t want to make any other patients hesitant to try medications. After all, we already know from my pharmacogenomics testing (click the link for great information) I have metabolisation issues with many medications (some too fast, some not at all, etc) – best not to use my personal experiences as an example of the efficacy of anything!
I actually don’t expect to achieve 100% of normal. My disease, psoriatic arthritis (PsA), like a lot of other chronic diseases, is A) not (yet) curable, and B) progressive. My patient understanding is that we hope to slow progression, not necessarily be able to stop it completely.
My rheumatologist (let’s call him Dr R) suggested I think about it like the Olympics – not everyone gets a gold medal, some people get silver. At the time, this sounded reasonable.
As I was walking the next day and thinking, always dangerous, I thought to myself, “Hang on a minute, in every race someone comes last!” And all the positions in between. Yes, every person who stands at the starting line hopes to get a gold medal, I know this, but only one does. I’m not sure this is the best analogy for Dr R to use. In fairness to Dr R, I think he came up with the Olympics on the fly, knowing my exercise strategy and thinking it fitted with the patient in question (me).
The initial three months have passed and yes, in the last two weeks I have started to feel much better. I have more energy, I found myself singing to the radio in the car (always a good sign) and my strength is slowly returning. At one stage I couldn’t lift my four litre saucepan if it was full, let alone do a six kilogram bicep curl. This was not just about strength – my hands and wrists were really sore if subjected to any load (saucepans or dumbbells), so although the biceps were quite happy, the wrists were not – we now have some improvement. I was waking every morning with my hands in a lot of pain and had difficulty bending my fingers (a complete reversal from when one hand had to be splinted to stop it locking into a fist). My hands are still a bit “grumpy” in the mornings, but at least they are usable!
The above photo was taken on October 22 – I wanted to wear an old bangle on a night out. As you can see, that wasn’t happening. My hands are still too swollen and the joint at the base of the thumb is bigger than it was in my pre-PsA days. So while I feel better overall than I did three months ago, am I “normal”? No. I think I might be at about 70% of normal taking into account my age which brings it’s own issues, irrespective of my PsA!
How could I measure it? Good question, I’m not sure. If I took the leg press as one measure, I am currently only doing 65 kg because I’m coming back from total knee replacement. My personal best since I was diagnosed is 160 kg. 65 is 40% of 160. But using that as a measure would be being unfair to the medication, as I am restricted in how much I can lift at the moment, being post-operative. I feel if it wasn’t for needing to be careful of my new knee, I could lift much more.
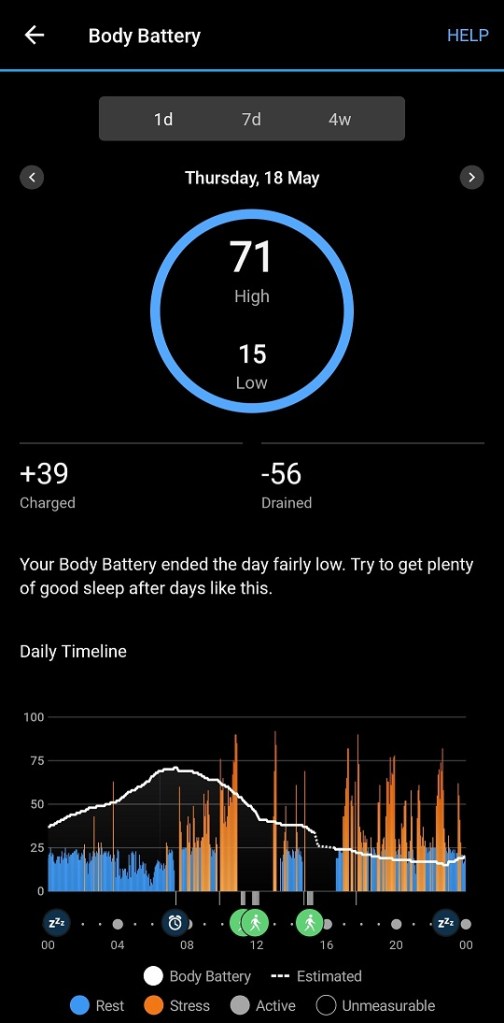
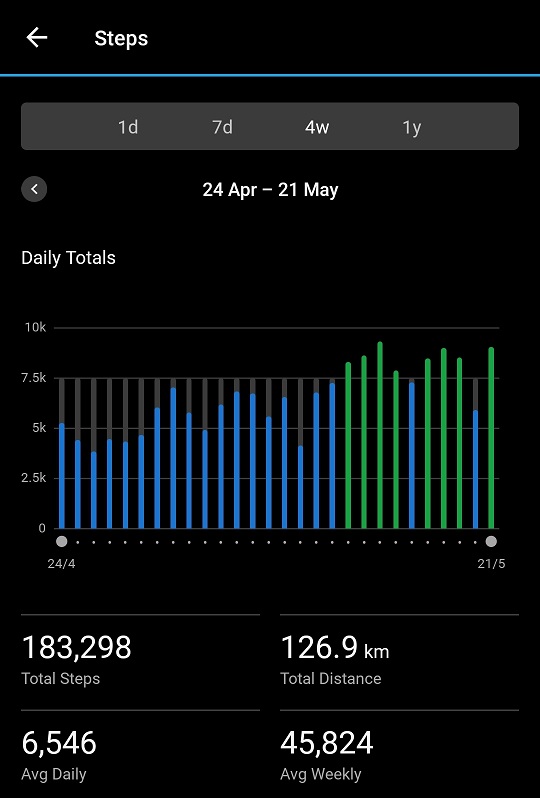
I’m not taking any pain medication other than Panadol Osteo, that’s a good measure, but I am supplementing with a low dose of NSAID as needed. I’m certainly doing more Movement As Medicine than I was before starting this medication: that is a very good sign. I’m writing (today at least).
Will I get the gold medal? I’m very wary of that as an analogy for treatment “success”. Too few people get gold medals in the sporting arena. How many of us come last? I know Dr R’s heart was in the right place, but I think expectations is something we perhaps need to look at more closely. What is a realistic expectation of improvement on any particular medication? Or, for that matter, with any particular condition?
As I stated above, this is my eighth medication since I was originally diagnosed in 2014 (with rheumatoid arthritis, later rediagnosed). That’s not counting the ever-present “extras” like NSAIDs and corticosteroids. But where am I in the race?
I think I know the answer: we don’t know! Personalised medicine is a rapidly developing field, but doesn’t cover everything yet. So I’ll keep running this race and hope I don’t end up last. Meanwhile, I’ll try to think of a better analogy. Maybe trying to hit sales targets? Not really my scene, but at least we’d stand an equal chance!
19/11/2023 Edited to clarify: by the phrase “So I’ll keep running this race and hope I don’t end up last” I mean I’m staying on this medication and hope improvements continue in the coming months. It occurred to me overnight that I may not have been very clear! My inflammatory markers were very nicely reduced too, which was good.