This article will not apply to all chronic illness patients: it is primarily applicable for those of us where specific parts of our body depend VERY MUCH on Movement As Medicine. In this article I am going to use my own recent example. Think about your own individual situation to determine if this may be a risk in your situation when surgery is looming.
Before we continue, a reminder about de-conditioning. In my case only one area of my body was feeling the affects as it was the part of the body I could not adequately maintain at home. Yes, I was doing biceps curls, shoulder press, chest press and several other exercises at home, but was not able to do the exercises required to adequately maintain full posterior chain strength. Given my small home, the weights above are all I have space for!

This issue will not apply to all surgeries either. It depends how long your post-op period is AND the degree of immobility required. For example, I’ve had both ankles fused. Same post-op period in both cases. However, with the left ankle I could drive four weeks earlier than with the right ankle and that four weeks, plus an additional, unrelated, hospitalisation, were enough to make what was, in my case, a major difference.
I have a rather troublesome lower spine (see 2025 MRI results below if interested in detail). Not a complete disaster, but bad enough that in 2017 I was offered radiofrequency denervation of the problem area as pain was radiating down my right leg. I elected to try improving my posterior chain strength instead. This has been very successful. Yes, there are still a couple of things that will irritate that area: bending (unless I religiously hinge at the hip) and standing motionless. Otherwise I can do anything I like pain-free.
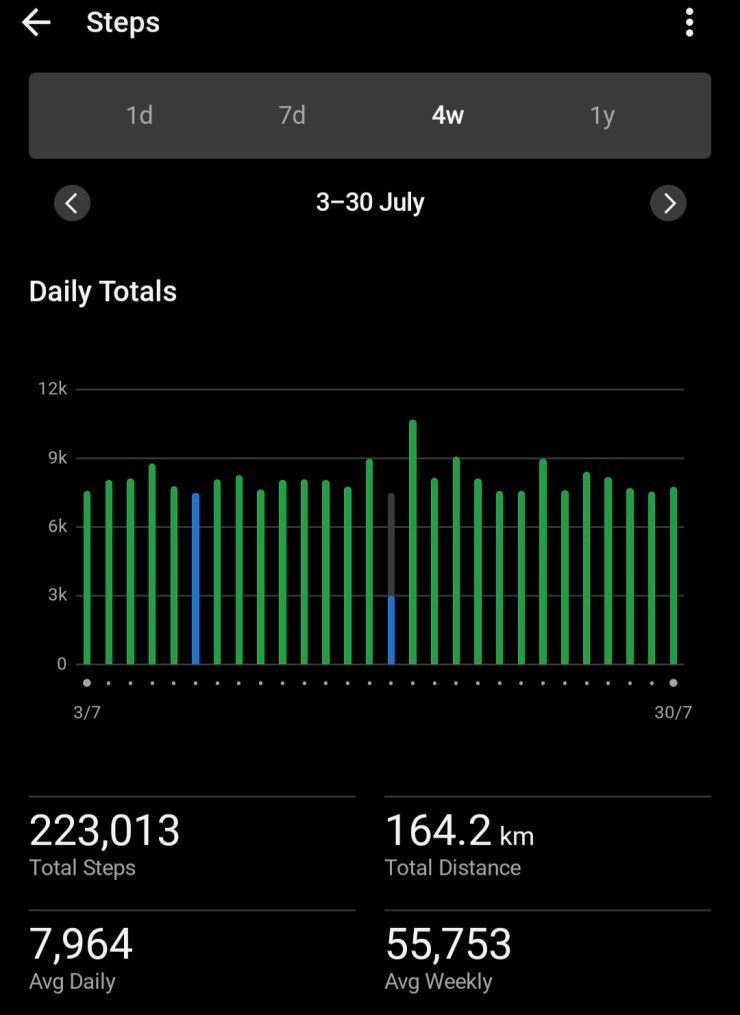
When I had the left ankle done in 2023, by the time I was in a moonboot and on crutches I could drive to the gym and do the weighted back exercises I needed to do to maintain my posterior chain strength. With the right ankle, obviously I couldn’t drive for an additional month. Then, two weeks after I could drive, I was back in hospital for a nasal/sinus infection. Essentially immobile again.
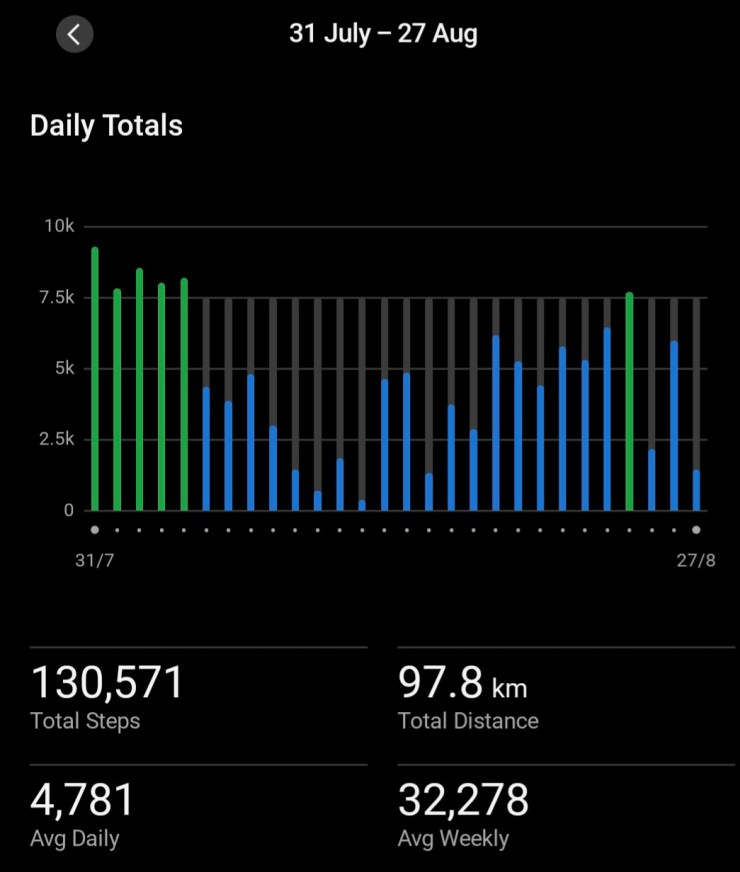
Once that was out of the way and I was back on my feet, I realised as I was walking that my posture was a disaster. I tried to stand up straight. Bottom line, I couldn’t. It wasn’t painful, I just could not straighten my back. I was horrified, as I knew this would not end well unless I did something about it.
Yes, I consulted my Exercise Physiologist and he gave me some specific rehab exercises to help. I increased (very carefully) my weight bearing posterior chain exercises. Now, almost a month after I detected the problem, I am almost back to where I was when I went in for surgery on December 2, 2025. I had not expected the de-conditioning to occur in that timeframe, although with hindsight, I should have.
Getting the situation corrected has not been painless. Mostly at the end of the day my lower back has expressed its discontent. There have been heat packs, Voltaren Gel, Panadol Osteo and a couple of days over that four weeks I have resorted to “the big guns”. However, I’ve reconditioned my back! Yay!
Knowing what I now know, what, if anything, could or would I do differently? To be perfectly honest, in this case there were not many options. Not have the surgery at all? Not an option! Had my foresight been working properly I would have taken a taxi to the gym twice a week to start the required exercises earlier. Not every patient can afford that option. In your own case, maybe enlist a family member to drive you to the gym. If you are really lucky you might have a gym in your basement!
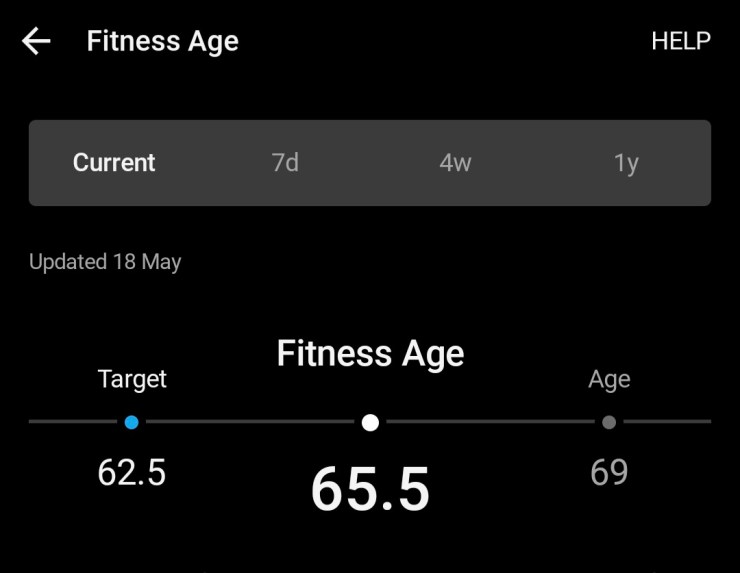
For me, even after nearly 12 years in this job of project managing my diseases, this was unexpected. Not to mention we de-condition faster the older we are. I’m now two years older than with the first ankle. My lower back issues have probably progressed over that time too.
As I said in my opening paragraph, this consideration will not apply to all chronic illness people or be a possible result of all surgeries. However, it is worth reviewing your situation pre-operatively to see if it MAY be an issue. It may not be the back: it could be a shoulder or any other part of the body that you are currently using Movement As Medicine to maintain. If you can’t maintain that work in the post-op period for a length of time, you may need to be prepared to work back up, as I have had to do. Practitioners such as Exercise Physiologists may be able to help you plan ways to minimise any issues.
In case readers are interested, these are the results of an August 2025 MRI of my Lumbar Spine. At the time they were looking for a possible infection. Thankfully none was found! Overall, not too bad! Just bad enough to be a bother if I don’t support it with good posterior chain strength.
MRI LUMBAR SPINE
FINDINGS:
No significant focal bony lesions or compression fractures are identified. There is a
moderate lumbar scoliosis convex to the left. No sign of spinal infection. Normal psoas
muscle. Sacroiliac joints are normal. Normal kidneys.
T12/L1: Normal
L1/L2: Normal disc. Moderate bilateral arthropathy
L2/L3: Tiny posterior disc protrusion and severe right-sided and moderate severe left-sided
arthropathy. No central canal stenosis. Moderate right bony foraminal narrowing
compressing the right L2 nerve.
L3/L4: Normal disc, severe right and moderate severe left facet joint arthropathy. Mild right
foraminal narrowing without nerve compression. No canal stenosis.
L4/L5: Slight posterior disc bulging and annular fissure. Severe bilateral arthropathy but
there is no central canal stenosis. Mild left bony foraminal narrowing. Normal right foramen
L5/S1: Normal disc. Moderately severe right and severe left facet joint arthropathy.
Synovial cyst projects posteriorly from the left facet joint. No central canal or foraminal
stenosis or nerve compression.
No facet joint fluid or inflammation
The conus and nerve roots of the cauda equina are normal. Paraspinal tissues are normal.
CONCLUSION:
No evidence of spinal infection. Multilevel degenerative change but no canal stenosis.