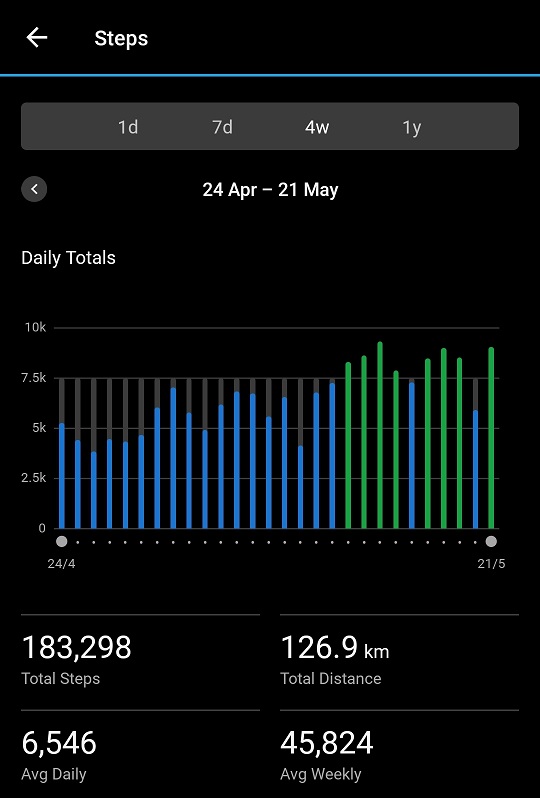
Above is a snapshot of my walks for the last four weeks. In my last article I wrote I was improving. Yet we see there was dip yesterday. Why is this so? You’ll be pleased to know it is a deliberate dip. A very deliberate dip, in fact. Recently I wrote Let’s Revisit Pacing. If you are new to my work I strongly suggest you click that link and read that first as this is, essentially, a sequel. A real life example.
Improvement has allowed me to get to the point I am walking 4 kilometres each day: but that was all I was doing! At least that was my primary use of energy over and above actually fueling the bodily functions that keep us alive: pumping blood, breathing, digesting food etc.
Yesterday I did two activities that require energy, that chew through our internal battery charge. I had a shower and I did grocery shopping. This wasn’t a “nip down to the shops and grab a pint of milk” trip, this was a monthly stock up. When I got back to my apartment it was four trips between my apartment and the car to bring everything inside. Then the effort of putting it all away.
When I initially wrote about what I call our internal battery, I stated I didn’t have a charge meter on my arm! I do now: my Garmin watch. Here it is for yesterday (Saturday) compared with Thursday. For whatever reason, I hadn’t charged my battery as well overnight Friday night, so I was already a little low on fuel Saturday morning. I will state I am not sure how accurate this is for chronically ill people – I’m working on watching it carefully – but it is certainly an indicator. Blue is charging your internal battery, orange is using it up.

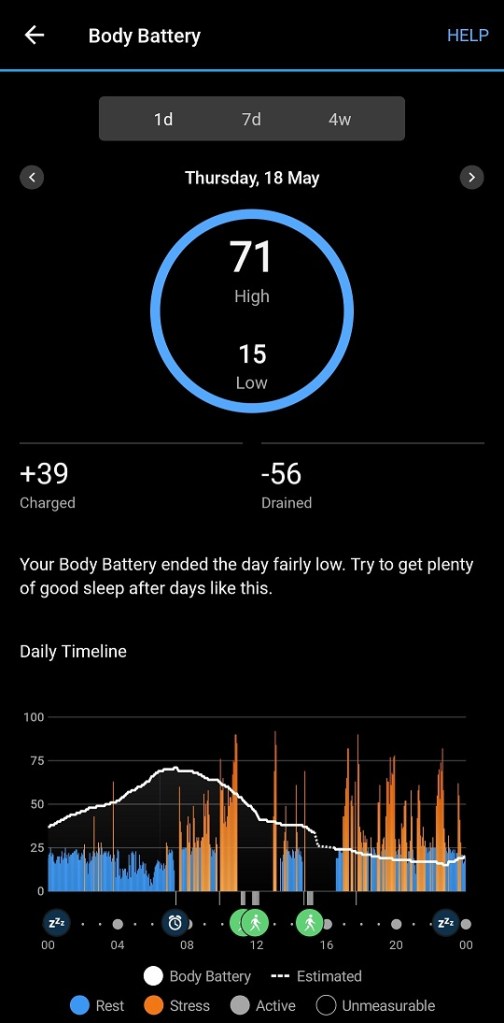
Another point to note is that most of the step counters will not register steps, or register steps accurately, if you are pushing a shopping trolley (or similar activity). Very annoying, as I think I walked about 1,000 steps just around the supermarket. Consequently there is also a dip in my steps for yesterday, even though I was moving. For those wondering the blue bars below are where I did not achieve my daily goal of 7,500 steps. Green bars are goal achieved!
Why not 10,000 steps you ask? Ahhh, well, yes, I have that covered too! Read We Need Personalised Numbers to understand the 10,000 figure is a myth.
Healthy people reading this will most likely understand shopping uses energy. They might raise an eyebrow over the shower taking energy. Trust me, for most of us chronically ill patients, a shower consumes energy. Many of us need a rest afterwards. I don’t usually, but I do at the moment.
What I did yesterday was adjusted my activities so that I did not Boom/Bust. I don’t need to burn through my internal battery one day then be wiped out for the following two or three days. Having a goal of 4 kilomtres a day is great, but at this stage of my “comeback” I am not risking any post exertional malaise (PEM). If I have to do something, like the grocery shopping, I will adjust my walking goal. Hopefully. in a few months I won’t need to: I’ll be back to my “normal”. Right at the moment, I’m not taking that risk. When I do head back to the gym for strength training, initially I will drop my walking goal for that day.
Using Movement As Medicine is not a simple “just get out there and walk”. It requires careful planning and monitoring. I hate “bust” days and monitor myself very carefully to avoid those days. Over time, following the pacing principles, I can do more. Pacing is the golden rule here! Today I walked 5 kilometres. I’ve been working up to it and I did nothing else that used energy today (other than writing this, of course).